Ulcerative colitis
Ulcerative colitis
Definition: Ulcerative colitis (UC) is a relapsing and remitting inflammatory condition of the large bowel, with unknown aeitiology.
Ulcerative colitis is moderately common with a prevalence of 100-200 per 100 000. It is 3 times more common than crohns, and is more common amongst Caucasians, and tends to affect women more than men. It has a bimodal distribution, most commonly affecting people between the ages of 15-30 with a smaller peak between 55-65.
Definition: Ulcerative colitis (UC) is a relapsing and remitting inflammatory condition of the large bowel, with unknown aeitiology.
Ulcerative colitis is moderately common with a prevalence of 100-200 per 100 000. It is 3 times more common than crohns, and is more common amongst Caucasians, and tends to affect women more than men. It has a bimodal distribution, most commonly affecting people between the ages of 15-30 with a smaller peak between 55-65.
Risk factors:
· Ulcerative colitis is thought to be
autoimmune
· Family history of parent, children
or sibling with ulcerative colitis increases the risk of an individual
developing it.
· Smoking is protective in ulcerative
colitis, and UC is 3 times more common in non smokers.


Presentation:
Ulcerative colitis tends to present with gradual onset of bloody diarrhea associated with cramping abdominal discomfort and increased bowel frequency.
Ulcerative colitis tends to present with gradual onset of bloody diarrhea associated with cramping abdominal discomfort and increased bowel frequency.
It may
present acutely with systemic symptoms including severe adominal pain and
diarrhea, fever, malaise, anorexia, and weight loss. Disease affecting the
rectum can also cause tenesmus (feeling like the need to empty bowels but being
unable to) and urgency.
Ulcerative colitis may also present with extraintestinal signs which includes:
Ulcerative colitis may also present with extraintestinal signs which includes:
- · Eye manifestations – episcleritis, scelritis and anterior uveitis
- · Clubbing
- · Apthtous ulcers
- · Enteropathic arthropathy( large joint mono or oligoarthropathy, or spondyloarthropathy or sacroilititis)
- · Clubbing
- · Erythema nodosum
- · Pyoderma gangrenosum
- · Liver disease- fatty liver, primary sclerosing cholangitis, cholangiocarcinoma
- · Renal stones (due to reduced absorption of fat which increases oxalate absorption and renal oxalate excretion causing oxalate sones)
- · Osteomalacia
- · Malnutrition
- · Amyloidosis
Examination findings
Patients with ulcerative colitis may have no signs on examination. In acute ulcerative colitis, patient may have a fever, with signs of dehydration (tachycardia, tachypnoea, dry mucous membranes etc). They may be anaemic, with pallor. They may also have a abdominal distension and tenderness.
Signs of extraintestinal disease may be present.
Differential diagnoses
Other causes of changes in bowel habits include:
Crohns
Patients with ulcerative colitis may have no signs on examination. In acute ulcerative colitis, patient may have a fever, with signs of dehydration (tachycardia, tachypnoea, dry mucous membranes etc). They may be anaemic, with pallor. They may also have a abdominal distension and tenderness.
Signs of extraintestinal disease may be present.
Differential diagnoses
Other causes of changes in bowel habits include:
Crohns
Infective
colitis (eg. C difficile infection)
Irritable
bowel syndrome (alarming symptoms such as blood in stools or night time urgency
not present)
Diverticular
disease
Colon
cancer (especially in older individuals)
Investigations
Bloods:
- FBC (may show anaemia, WCC may be raised in toxic megacolon), ESR and CRP (raised), urea and electrolytes (dehydration may cause abnormalities), Liver function tests (albumin levels sometimes drop). Iron studies, B12 and folate may also be appropriate.
- Serum antibodies – pANCA is associated with UC.
- Stool microscopy and cultures – to exclude infections – eg. C difficile, salmonella, shigella etc. patients with inflammatory bowel disease may have a higher prevalence of C. diff infections, so its presence does not rule out diagnosis.
- Faecal calprotectin – shows colonic inflammation, may differentiate this from irritable bowel syndrome.
Imaging:
- Abdominal x ray may show colonic dilatation with mucosal thickening/islands which may indicate toxic megacolon.
- Chest x ray may show gas under the diaphragm in a perforation.
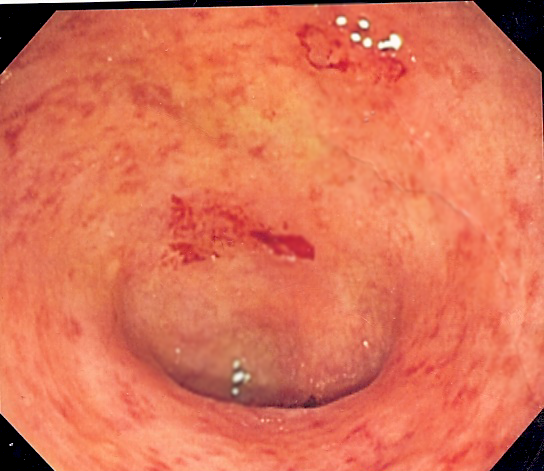
- Sigmoidoscopy and rectal biopsy
- Colonoscopy – gold standard for diagnosis but may increase risk of bowel perforation in moderate to severe disease.
- Do not do barium enemas during severe acute attacks or to diagnoses UC.
Other
investigations may include:
ultrasound, CT, MRI, radionuclide scanning.
ultrasound, CT, MRI, radionuclide scanning.
Management
Ulcerative
colitis can be categorized into mild, moderate or severe disease based on the
Truelove and Witts severity index in adults or the pediatric ulcerative colitis
activity index in children.
mild
|
moderate
|
Severe
|
Less than
4 stools a day, little rectal bleeding, apyrexia (measured at 6am), with a
pulse rate less than 70. ESR less than 30mm/h and haemoglobin over 11g.DL
|
4-6
stools a day with moderate blood in stools. Low grade or no fever (37.1-37.8
ºC) with a pulse of 70-90. Haemoglobin
between 10.5-11g/dL and normal ESR and CRP.
|
6 or more
stools a day with visible blood in stools. Signs of systemic illness
including fever over 37.8ºC, pulse over 90bpm, anaemia with Hb under 10.5g/dL
and raised ESR (over 30mm/h) or CRP
|
Management of ulcerative colitis depends on the severity of the disease at presentation. Although it should be managed through a multidisciplinary team in the long run, with appropriate patient education.
Patient should be admitted to hospital if:
- · They have signs and symptoms of severe ulcerative colitis
- · They have moderate UC which does not respond within 2 weeks
Medical management (based on NICE guidiance)
Mild- moderate ulcerative colitis affecting the anus or anus and sigmoid only
Offer topical aminosalicylates (eg. mesalazine) as first line to induce remission, adding oral aminosalicyclate or treating with only oral aminosaicyclate if necessary.
Mild- moderate ulcerative colitis affecting the anus or anus and sigmoid only
Offer topical aminosalicylates (eg. mesalazine) as first line to induce remission, adding oral aminosalicyclate or treating with only oral aminosaicyclate if necessary.
Topical
corticosteroids or oral prednisolone can be used to induce remission where aminosalicyclate
cannot be used.
Consider
adding oral prednisolone to aminosalicylate to induce remission if no
improvement is seen after 4 weeks or symptoms worsen. Consider adding
tacrolimus where oral prednisolone is ineffective.
Aminosalicylate can be used to maintain remission. This is most effective if it is given topically, or as a combination of an oral medication and topical medication. New aminosalicylates have less side effects but are thought to be less effective and more expensive.
Aminosalicylate can be used to maintain remission. This is most effective if it is given topically, or as a combination of an oral medication and topical medication. New aminosalicylates have less side effects but are thought to be less effective and more expensive.
Azathioprine
and mercaptopurine can be used to maintain remission where frequent
exacerbations of ulecerative colitis occurs requiring corticosteroids (more
than 2 episodes per year) or if aminosalicylates are ineffective at maintaining
remission.
Extensive mild-moderate ulcerative colitis
Extensive mild-moderate ulcerative colitis
Offer high
dose oral aminosalicylate as first line treatment for inducing remission.
Considering adding topical aminosalicylate or oral beclomethasone dipropionate.
Use oral prednisolone where aminosalicyclates are contraindicated.
Use oral prednisolone where aminosalicyclates are contraindicated.
Offer oral
aminosalicylate to maintain remission. Again azathioprine and mercaptopurine
can be used as second line drugs.
Acute severe ulcerative colitis
Acute severe ulcerative colitis
Acute
severe UC should be managed by the gastroenterologists and colorectal surgeons,
via a multidisciplinary team. Patient should be resuscitated with IV fluids and
be nil by mouth. The patient should have regular obs and a stool chart, and be
examined twice daily. Bloods should be repeated daily with abdominal xray if
necessary. IV corticosteroids should be used first line to induce remission,
and the need for surgery should be assessed.
Consider
ciclosporins second line or surgery if IV corticosteroid are contraindicated or
not tolerated. Ciclosporins can also be used if symptoms worsen or if no
improvement is seen after 72 hours. Ciclosporin has a high toxicity with a mortality
rate of 3% and should be considered carefully before use.
Infliximab
can also be considered where ciclosporins are contraindicated.
Maintenance
of remission is same as mild-moderate UC (with topical or oral aminosalicyclate
depending on the extent of the disease).

Surgical management:
Colectomy or proctocolectomy will treat ulcerative colitis where it cannot be managed medically or due to colon cancer.
Complications:
Perforation
Colectomy or proctocolectomy will treat ulcerative colitis where it cannot be managed medically or due to colon cancer.
Complications:
Perforation
Bleeding
Toxic
megacolon
Increased
colonic cancer risk (about twice of general population) – screening via
colonoscopy in high risk groups is available.
Prognosis
Ulcerative colitis is a chronic condition and is associated with reduced life expectancy. About 20% of patients will require surgery at some stage in their illness.
Prognosis
Ulcerative colitis is a chronic condition and is associated with reduced life expectancy. About 20% of patients will require surgery at some stage in their illness.



Comments
Post a Comment