Subarachnoid haemorrhage
Definition and demographics:
A subarachnoid haemorrhage refers to the spontaneous arterial bleeding into the subarachnoid space, usually from berry aneurysms in the circle of willis. It is relatively rare, with an average GP seeing one case every 7 years, although it makes up 6% of all strokes. It tends to affect younger patients compared to other types of strokes, with a mean age of 50.
Pathophysiology and aetiology:
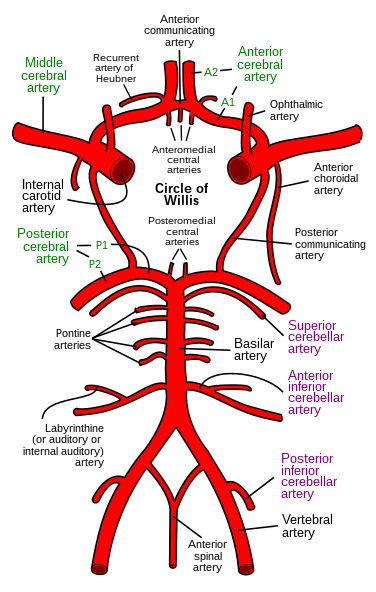
Subarachnoid haemorrhages are caused by the rupture of berry aneurysms developing on the circle of willis.
These are most common between the posterior communicating artery and the internal carotid artery, between the anterior communicating artery and the anterior cerebral artery, and at the tri- or bifurcation of the middle cerebral artery. The formation of berry aneurysms is thought to be partly due to genetical pre deposition affecting the tissues of the vessels and additional strains such as hypertension and atherosclerosis.
Other causes of subarachnoid haemorrhages include arteriovenous malformations, and rarer causes such as bleeding disorders, meningitis, tumours, arteritis, marfans and Ehlers-Danlos syndrome, and polycystic kidneys.
Risk factors:
Increasing size of the aneurysm (aneurysms <7mm are="" p="" rupture="" to="" unlikely="">
Hypertension
Smoking
Excessive alcohol intake
Genetical predisposition
Family history
Autosomnal dominant adult polycystic kidney disease
Presentation:
- Sudden severe headache lasting for a few seconds or a fraction of a second.
- Headache may persist for 1-2 weeks.
- Usually diffuse.
- Tends to be severe - most severe ever experienced
- Seizures are rare, but are highly suggestive of a bleed.
- This may be followed by vomiting and loss of consciousness then death.
Most patients will have a depressed level of consciousness on admission. Neck stiffness may be present, kernig's sign may be positive, and papilloedema, or retinal haemorrhage may be present. Blood pressure may also be raised.
Differential diagnosis: Migraine, Tunderclap headache, meningitis with microabcess rupture causing a sudden headache. Cervical arterial dissection.
Investigations
Urgent CT is the primary investigation needed, which may show blood in the subarachnoid space or the ventricles. Lumbar puncture should be done to rule out a SAH if the CT scan is doubtful- this should be done 6-12 hours after the episode to allow the haemoglobin to degrade, unless there are other indications. The CSF becomes yellow several hours after a bleed. Inspection of the CSF is usually enough to diagnose an SAH but spectrophotometry may be used to measure the bilrubin in the CSF.
MRI or CT angiography may be done prior to any surgery.
Management
SAH is managed medically initially, with bed rest and supportive care. Nimodipine, a calcium channel blocker is prescribed and reduces spasm. Patients should be monitored for electrolyte changes and hypertension should be corrected. Patients should be referred to a specialist neurosurgical centre.
Interventions to prevent rebleeding is done once the patient is stable. This includes neurosurgical clipping, endovascular coiling. In addition, nimodipine and anti platelets may be given to reduce the risk of cerebral ischaemia.
Complications: The blood in the subarachnoid space may cause an obstructive hydrocephalus. In addition, arterial spasm may occur and cause coma or hemiparaesis.
Prognosis: If untreated, patients are likely to rebleed. Up to 15 % of patients rebleed within the first day and 40% within 4 weeks. Up to half of patients will die within 3 weeks of a subarachnoid haemorrhage, and a 1/3rd of the survivors will become dependent.
References:
References:
Kumar P, Clark M, eds. Kumar and Clark's Clinical Medicine, 7th Ed. Edinburgh, Saunders Elsevier, 2009.
http://www.patient.co.uk/doctor/subarachnoid-haemorrhage
http://www.bmj.com/content/339/bmj.b2874
http://en.wikipedia.org/wiki/File:Circle_of_Willis_en.svg
http://en.wikipedia.org/wiki/File:Circle_of_Willis_en.svg



Comments
Post a Comment