Occular melanoma
Definition and demographics
Occular melanomas are uncontrolled malignant proliferation of melanocytes in the eye. They can be divided into uveal melanomas, which arise in the iris, choroid body or ciliary body, and conjunctival melanomas which arise from the conjunctiva. Uveal melanomas are more common and is the most common type of primary eye malignancy, and second most common type of malignant melanoma.
Ocular melanoma is a rare condition which occurs equally in males and females and the with a peak incidence in people's 60s. It tends to affect fair skinned individuals more.
Aeitiology/pathophysiology
Occular melanomas are caused by an accumulation of genetic changes. Sunlight exposure is a risk factor of developing melanoma. Other risk factors include being caucasion/fair skinned, having light coloured irides, melanosis or existing melanocytic naevi of the conjunctiva (moles), congenital ocular melanocytosis, neurofibromatosis and family history.

Presentation:
Occular melanoma may cause local symptoms depending on the position of the tumour. However it may also be asymptomatic, or only present with symptoms due to distal metastases.
Common complaints include:
Partial loss of visual field
Sun sensitivity
Blurred vision
Incidental finding on eye examination
Other local symptoms include a protruding eye, change in iris colour, or a red painful eye.
Systemic complaints such as weight loss, tiredness, and changes in bowel or bladder habits may be caused by distal metastases.
Clinical examination:
Occular melanomas affecting the conjunctiva or iris may be visible without fundoscopy
 |
| Melanoma of the iris |
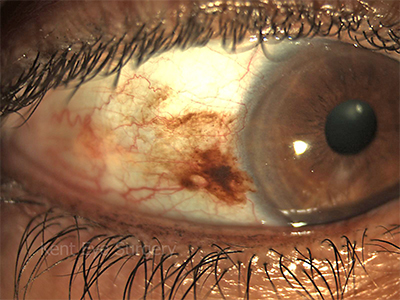 |
| Conjunctival melanoma |
Loss of visual acuity ± visual field defects
On fundoscopy - there may be a nodular dome shaped lesion on fundoscopy. occasionally a diffuse lesion growing laterally may be seen. The lesions vary in colour but may be a melanotic.
Occasionally inflammation marked by inflammatory cells in the vitreous may be seen, haemorrhages or hyhaema (blood in the anterior chamber of the eye), or retinal detachment may be seen.
Advanced disease may also cause exophthalmos of the eye.
 |
| Choroidal melanoma |
Differential diagnoses
Choroidal nevus (benign melanocytic tumour)
Melanocytoma (benign melanocytic tumour)
Metastases from non-ocular tumour
Choroidal detachment
Intra-ocular foreign body
Cavernous haemangioma
Exudative retinal detachment of another cause
Wet macular degeneration
Retinoblastoma (younger patients)
Glaucoma
Sarcoidosis
Tuberculosis
Investigations and diagnosis
Fundoscopy with funds imaging
Ultrasound scan of the eye - Used to establish diagnosis, evaluate if the tumour extends beyond the eye, to determine size and to observe tumour.
CT and MRI of the eyes is usually less sensitive (i.e. higher number of false positive results) however they may be useful in determining extraoccular involvement.
Fine needle biopsy may be performed if diagnosis is doubtful, especially in amelanotic lesions, incisional biopsy should not be used due to increased risk of recurrence and metastases.
Liver function test- if abnormal liver metastases may be present, and further imaging may be required.
Liver ultrasound scan or CT - to look for liver metastases
PET-CT scan - to look for metastases
CXR - rule out lung metastases
Management
Staging - for choroidal melanomas
Classified by anatomical origin, growth pattern (dome shaped vs diffuse), location around optic nerve or macular, and size (based on thickness and size. (<10mm 10-15="" medium="" small="">15mm large)
Observation may be appropriate initially for where diagnosis is not well established.
Plaque radiotherapy and surgical resection are used to treat medium sized melanomas.
Conjunctival melanomas are treated by wide local excision with adjuvant therapy which may be in the form of brachytherapy, cryotherapy, or topical chemotherapeutic agent.
Occular melanoma primarily spreads either locally, or primarily to the liver. Other location for metastases include the lungs, bones and the central nervous system. Metastases can be treated in the liver with melphalan, or surgical resection. Ipilumumab may also be effective and internal radiation therapy may also be effective.
Prognosis
Occular melanomas tend to present quite late. Metastases tends to occur in 40-50% of cases by 5 years. And 50% of patients die within 10 years from diagnosis. Death is usually due to metastatic disease. Certain characteristics of the tumour may lead to worse prognosis.



Comments
Post a Comment